Candy Land Was Invented for Polio Wards - The Atlantic
Candy Land Was Invented for Polio Wards - The Atlantic |
| Candy Land Was Invented for Polio Wards - The Atlantic Posted: 28 Jul 2019 05:00 AM PDT  If you were a child at some point in the last 70 years, odds are you played the board game Candy Land. According to the toy historian Tim Walsh, a staggering 94 percent of mothers are aware of Candy Land, and over 60 percent of households with a five-year-old child own a set. The game continues to sell about a million copies every year. You know how it goes: Players race down a sinuous but linear track, its spaces tinted one of six colors or marked by a special candy symbol. They draw from a deck of cards corresponding to the board's colors and symbols. They move their tokens to the next space that matches the drawn color or else teleport to the space matching the symbol. The first to reach the end of the track is the winner. Nothing the participants say or do influences the outcome; the winner is decided the second the deck is shuffled, and all that remains is to see it revealed, one draw at a time. It is a game absent strategy, requiring little thought. Consequently, many parents hate Candy Land as much as their young kids enjoy it. Yet, for all its simplicity and limitations, children still love Candy Land, and adults still buy it. What makes it so appealing? The answer may have something to do with the game's history: It was invented by Eleanor Abbott, a schoolteacher, in a polio ward during the epidemic of the 1940s and 1950s. Read: How a bad night's sleep birthed the sound conditioner The outbreaks had forced children into extremely restrictive environments. Patients were confined by equipment, and parents kept healthy children inside for fear they might catch the disease. Candy Land offered the kids in Abbott's ward a welcome distraction—but it also gave immobilized patients a liberating fantasy of movement. That aspect of the game still resonates with children today. Poliomyelitis—better known as polio—was once a feared disease. It struck suddenly, paralyzing its victims, most of whom were children. The virus targets the nerve cells in the spinal cord, inhibiting the body's control over its muscles. This leads to muscle weakness, decay, or outright fatality in extreme cases. The leg muscles are the most common sites of polio damage, along with the muscles of the head, neck, and diaphragm. In the last case, the patient would require the aid of an iron lung, a massive, coffin-like enclosure that forced the afflicted body to breathe. For children, whose still-developing bodies are more vulnerable to polio infection, the muscle wastage from polio can result in disfigurement if left untreated. Treatment typically involved physical therapy to stimulate muscle development, followed by braces to ensure the affected parts of the body retained their shape. Vaccines appeared in the 1950s, and the disease was essentially eradicated by the end of the millennium. But in the mid-century, polio was a medical bogeyman, ushering in a climate of hysteria. "There was no prevention and no cure," writes the historian David M. Oshinsky."Everyone was at risk, especially children. There was nothing a parent could do to protect the family." Like the outbreak of AIDS in the 1980s, polio's eruption caused fear because its vectors of transmission were poorly understood, its virulence uncertain, and its repercussions unlike other illnesses. Initially, polio was called "infantile paralysis" because it struck mostly children, seemingly at random. The evidence of infection was uniquely visible and visceral compared to infectious diseases of the past, too. "It maimed rather than killed," as Patrick Cockburn puts it. "Its symbol was less the coffin than the wheelchair." Children of the era faced an unenviable lot, whether infected with polio or not. Gerald Shepherd provides a glimpse of the paranoiac atmosphere of the polio scare and its effects on children in a firsthand account of his San Diego childhood in the late 1940s, at the height of the polio epidemic. Quarantine and seclusion were the most common preventative measures:
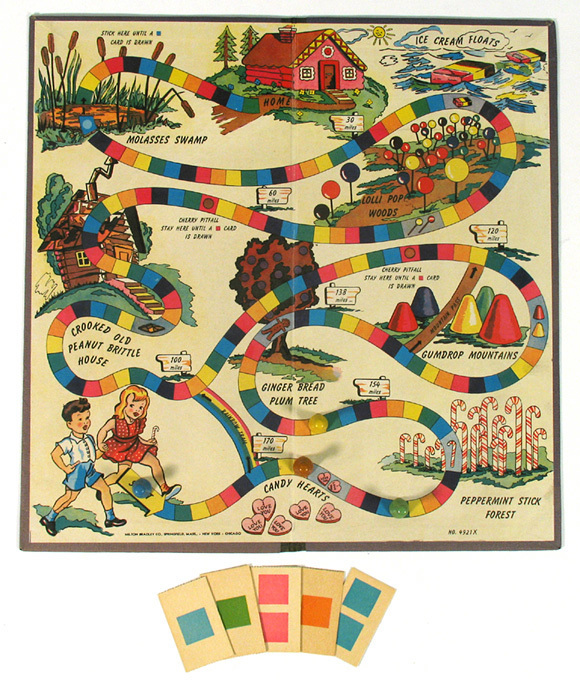
Kids his age were well aware of what polio could do: "Every time one of our buddies got sick," Shepherd recollects, "we figured he was headed for the iron lung." If you caught polio, you would be committed to a hospital with a chance of being forever anchored to a machine. If you didn't catch it, you would be stuck indoors for the foreseeable future (which, from a child's perspective, might as well be forever). For a child of the 1940s or '50s, polio meant the same thing whether you contracted it or not: confinement. The Milton Bradley executive Mel Taft has said Eleanor Abbott, the inventor of Candy Land, was "a real sweetheart," whom he liked immediately. According to Walsh, the two met when Abbott brought Milton Bradley a Candy Land prototype sketched on butcher paper. "Eleanor was just as sweet as could be," Taft recalled. "She was a schoolteacher who lived in a very modest home in San Diego." Details about her life outside this interaction are scant. Curators at the Strong Museum of Play in Rochester, New York, say that the museum has no holdings in its extensive archives from Abbott's records; they rely on Walsh's account. Walsh told me that Taft was his only source, and Hasbro, which now owns Milton Bradley, did not respond to a request for records that might verify Abbott as the game's inventor. Among the few facts researchers have unearthed about her: A phone book containing her number exists in the collections of the San Diego Historical Society (the only trace of her in their archives). And according to some accounts, she gave much of the royalties she earned from Candy Land to children's charities. There is reason to believe Abbott was ideally suited to consider polio from a child's perspective. As a schoolteacher, she would have been acquainted with children's thoughts and needs. And in 1948, when she was in her late 30s, she herself contracted the disease. Abbott recuperated in the polio ward of a San Diego hospital, spending her convalescence primarily among children. Imagine what it must have been like to share an entire hospital ward with children struggling against polio, day after day, as an adult. Kids are poorly equipped to cope with boredom and separation from their loved ones under normal circumstances. But it would be even more unbearable for a child confined to a bed or an iron lung. That was the context in which Abbott made her recovery. Read: What America looked like: Polio children paralyzed in iron lungs Seeing children suffer around her, Abbott set out to concoct some escapist entertainment for her young wardmates, a game that left behind the strictures of the hospital ward for an adventure that spoke to their wants: the desire to move freely in the pursuit of delights, an easy privilege polio had stolen from them. From today's perspective, it's tempting to see Candy Land as a tool of quarantine, an excuse to keep kids inside in the way Shepherd remembers. The board game gathers all your children in one place, occupying their time and attentions. Samira Kawash, a Rutgers professor, suggests that this is the main way polio informed the game's development: "The point of Candy Land is to pass the time," she writes, "certainly a virtue when one's days are spent in the boring confines of the hospital and an appealing feature as well of a game used to pass the time indoors for children confined to the house." For Kawash, Candy Land justifies and extends the imprisonment of the hospital, becoming another means of restriction. But the themes of Candy Land tell a different story. Every element of Abbott's game symbolizes shaking off the polio epidemic's impositions. And this becomes apparent if you consider the game's board and mechanics relative to what children in polio wards would see and feel. 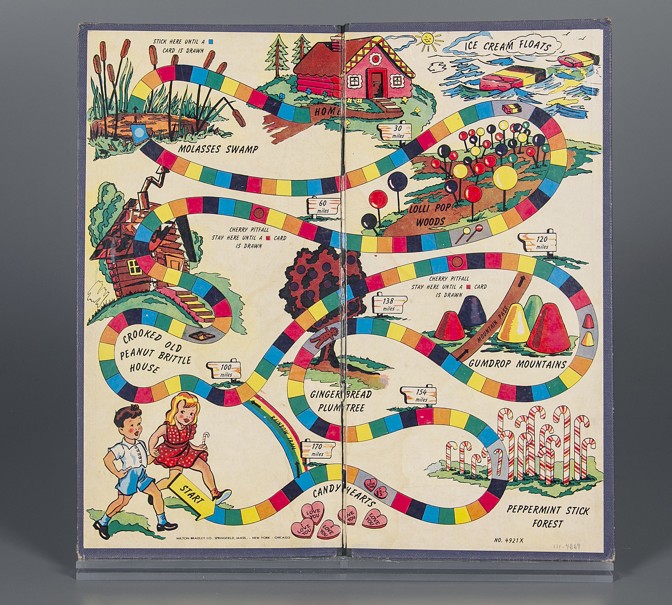 In 2010, when he was almost 70 years old, the polio survivor Marshall Barr recalled how only brief escapes from the iron lung were possible: "[The doctors] used to come and say, 'You can come out for a little while,' and I used to sit up perhaps to have a cup of tea," he writes, "but then they would have to keep an eye on me because my fingers would go blue and in about 15 minutes I would have to go back in again." Children would have played Abbott's early version of Candy Land during these breaks, or in their beds. Walsh, the toy historian, reports that kids loved Abbott's game, and "soon she was encouraged to submit it to Milton Bradley." In part, anything that would reduce boredom would have excited kids during treatment. As the historian Daniel J. Wilson explains, the wards provided little to occupy their young occupants. "In most cases, patients had to find ways to entertain themselves," he writes. Read: The invasion of German board games It was a tall order. The ward's setup taxed the imagination. The staff, fellow patients, or radio broadcasts would have been a child's sole company—only doctors and nurses were allowed allowed in the room. Images of polio wards depict a geometry even more rigid and sterile than typical hospital settings: row upon row of treatment beds and iron lungs. The children lying supine in iron lungs could only see what was on either side of their heads (a line of patients telescoping down the ward) or reflected in mirrors mounted overhead (the floor's tessellation of bleached tiles). Candy Land offered a soothing contrast. Repeating tiles line the game's board, but instead of a uniform, regimented grid, Abbott rearranges them into a meandering, rainbow ribbon. Even tracing it with your eyes is stimulating—an especially welcome feature if illness has rendered them the most mobile part of your body.  A colorful chocolate and candy landscape seems like the game's main attraction, but Candy Land's play revolves around movement. In theme and execution, the game functions as a mobility fantasy. It simulates a leisurely stroll instead of the studied rigor of therapeutic exercise. And unlike the challenges of physical therapy, movement in Candy Land is so effortless, it's literally all one can do. Every card drawn either compels you forward or whisks you some distance across the board. Each turn promises either the pleasure of unencumbered travel, or the thrill of unexpected flight. The game counters the culture of restriction imposed by both the polio scare and the disease itself. Read: How board games conquered cafes The joy of movement, especially for polio patients, seems to have been integral to Abbott's design philosophy from the start. The original board even depicts the tentative steps of a boy in a leg brace. The game also recognizes that mobility entails autonomy. At least part of Candy Land's appeal is the feeling of independence it provides its young players. In a backstory printed in the game's instruction manual, the player tokens (in the current edition, four brightly colored plastic gingerbread men) are said to represent the players' "guides." It represents their chance to be an active agent, with assistance—an ambulatory adventurer, not a prisoner of the hospital or home. It may even mark the first time they feel like a protagonist. The threat of polio has lessened over time, but Candy Land's value persists because of what it teaches. This is not to rehash the usual litany of early childhood skills some Candy Land proponents tout. Yes, the game strengthens pattern recognition. Sure, it can teach children to read and follow instructions. In theory, it shows children how to play together—how to win humbly or lose graciously. But any game could teach these skills. Candy Land's lessons are not to be found in the game, but in its results. Now that polio is a distant fear and mobility a power taken for granted, most games of Candy Land disappoint. The rules today are the same as they were in 1949, but something about the proceedings simply does not add up. Eventually, children recognize that they don't have a hand in winning or losing. The deck chooses for them. An ordained victory is an empty one, without the satisfaction of triumph through skills or smarts. When children want a more challenging experience, they leave Candy Land behind. And that, in the end, is what makes Candy Land priceless: It is designed to be outgrown. Abbott's game originally taught children to envision a world beyond the polio ward, immobilized and separated from family, where opportunities for growth and adventure could still materialize. Today, that lesson persists more broadly. The game teaches children that all arrangements have their alternatives. It's the start of learning how to imagine a better world than the one they inherited. As it has done for generations prior, Candy Land continues to send young children on the first steps of that journey. This post appears courtesy of Object Lessons. We want to hear what you think about this article. Submit a letter to the editor or write to letters@theatlantic.com. Alexander B. Joy is a writer based in New Hampshire. |
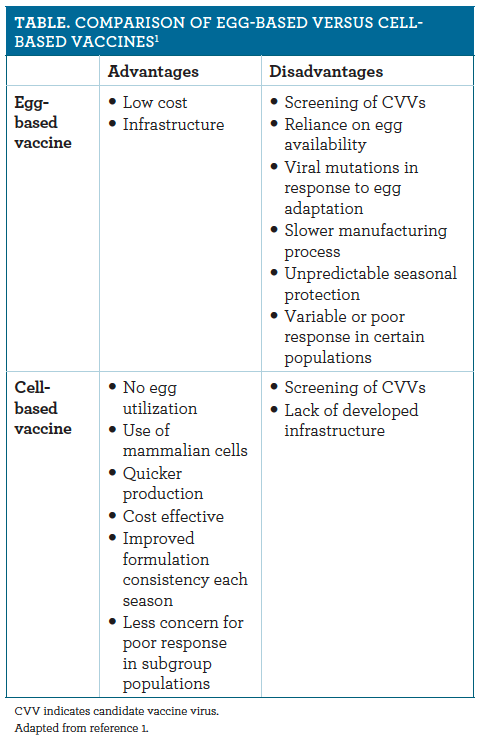
| Posted: 28 Jul 2019 11:00 AM PDT W. Justin Moore, PharmD; and Anooj Shah, PharmD A dvancing technology in vaccine development has allowed for the production of cell culture–based vaccines for illness such as chickenpox, rotavirus, polio, smallpox, hepatitis, rubella, and most recently influenza (flu). Cell-based vaccines have many potential advantages (see Table1), one of which includes longer stability and more rapid manufacturing, as cellbased vaccines can be frozen and used at a later date, with dependable cell lines to ensure consistent supply. Cell-grown, cell-based candidate vaccine viruses (CVVs) more similarly resemble circulating flu viruses; in contrast, egg-adapted alternatives may result in production of antibodies that less effectively prevent specific flu viruses.2 Additionally, cell-based vaccine formulations are preservative-free and present less concern for viral mutations caused by the egg-based vaccine production (which, in turn, can cause less effective immune responses to flu viruses). Avoidance of traditional manufacturing processes may also help reduce the risk of adverse reactions in patients with egg allergies.
Since the advent of increased legislation and funding in 2005, cell-based vaccine development has been a priority for US pandemic influenza preparedness.3 As a result, cell-based influenza vaccine development has rapidly advanced. Traditional egg-based vaccines face limitations such as a reliance on an adequate global egg supply, the inability to ramp up manufacturing quickly, a long production process, and the potential for mismatch with influenza strains based on antigenic variations. Cell-based vaccine development processes include a quicker production cycle, which, again, may reduce the time necessary to implement widespread vaccination efforts in the face of a potential epidemic. Cell-based influenza vaccines are grown via cultured cells of mammalian origin rather than in hens' eggs, as has been usual. Cell-based vaccines are produced via inoculation of CVVs with selection recommendations from the World Health Organization (WHO).2 These are grown in cultured animal cells and given time to replicate. Following replication, virus-containing fluid is isolated from cells and virus antigen is purified. The virus antigen then undergoes testing and approval processes through the FDA. Cell-based vaccines do not rely on the animal production and farming processes that are required for egg-based vaccines.3 This cell-based vaccine process was approved by the FDA in 2012, and production of Flucelvax, the sole cell-based influenza vaccine available in the United States, began in August 2016. Flucelvax's approval was based on a clinical trial conducted in Europe and United States which included more than 11,404 participants who were randomized to receive Flucelvax (n = 3828), Agriflu (n = 3676), or placebo (n = 3000). The results of the clinical trial indicated that Flucelvax was 83.8% effective in preventing influenza infection compared with placebo and was noninferior to the egg-based vaccine, Agriflu.4 As additional support for the vaccine's effectiveness, a retrospective study, which included data from more than 13 million Medicare beneficiaries aged 65 years and older during the 2017-2018 H3N2-dominated flu season, compared the effectiveness of Flucelvax with egg-based quadrivalent, egg-based high-dose, adjuvant, and standard-dose vaccines. Of the 13 million participants, 5% received a cell-based quadrivalent, 14% received an egg-based quadrivalent, 63% received a high-dose vaccine, 11% received an adjuvant, and 7% received the standard trivalent. The results indicated that the cell-based vaccines were approximately 11% more effective in preventing flu-related hospital admissions and clinic visits compared with the egg-based vaccines.4 Although this finding was not statistically significant, the reduction in hospital admissions and clinic visits was likely clinically significant. Vaccine efficacy measured by titers is another method to evaluate effectiveness of various vaccine formulations. Investigators have explored titerresponse between cell-based and egg-based vaccine preparations. In 2018, Rajaram et al conducted a retrospective evaluation of vaccine effectiveness comparing egg-based and cell-based isolations of influenza strains; this was based on data that was collected about antigenic similarity between mammalian cell– based versions and egg-based versions of the H3N2 viruses, and on measured titers using hemagglutination inhibition assays. After analyzing the data, the investigators found that a higher proportion of the H3N2 virus samples matched the mammalian reference compared with the egg-based reference. The low level of antigenic similarity between the H3N2 virus and egg-based reference may explain the relatively low effectiveness of eggbased vaccines against the H3N2 strain.5 In April 2019, Seqirus announced its decision to manufacture Flucelvax Quadrivalent for the 2019-2020 season using the cell-based approach that is recommended by the WHO. The decision was based on the decreased vaccine effectiveness of egg-based vaccines against the H3N2 strain found by Rajaram et al. The 2019-2020 vaccine formulation includes the following 4 strains: (1) A/Singapore/GP1908/2015 IVR-180 (H1N1) (an A/Michigan/45/2015-like virus); (2) A/North Carolina/04/2016 (H3N2) (an A/Singapore/INFIMH-16-0019/2016-like virus); (3) B/Iowa/06/2017 (a B/Colorado/06/2017-like virus); and (4) B/Singapore/INFTT-16-0610/2016 (a B/Phuket/3073/2013- like virus).6-9 Cell-based vaccine technology is an encouraging advancement that should allow more people to receive more effective and more timely flu vaccines. The widespread use of cell-based vaccines may prove to offer additional benefits as well, such as decreased hospitalization and health care–associated costs for patients, among the other potential advantages discussed. Further research is warranted to help quantify the impact of cell-based vaccines on clinical outcomes. W. JUSTIN MOORE, PHARMD is currently completing his PGY-1 residency training at Northwestern Memorial Hospital where he will also complete his PGY-2 infectious diseases residency. ANOOJ SHAH, PHARMD is currently completing his PGY-1 residency training at Northwestern Memorial Hospital where he will also complete his PGY-2 infectious diseases residency. REFERENCES
|
| You are subscribed to email updates from "polio prevention" - Google News. To stop receiving these emails, you may unsubscribe now. | Email delivery powered by Google |
| Google, 1600 Amphitheatre Parkway, Mountain View, CA 94043, United States | |



{kind=link}
{kind=link}
Comments
Post a Comment