polio history
polio history |
- The Virus Research of Jonas Salk Led to Polio Vaccine - Pharmacy Times
- Throwback Thursday: When Winona started saying goodbye to polio - Winona Daily News
- HISTORY, Feb. 23: US begins mass inoculations against polio - StarNewsOnline.com
- This Is the Truth About Vaccines - The New York Times
- Polio this week as of 6 March 2019 - Afghanistan - ReliefWeb
| The Virus Research of Jonas Salk Led to Polio Vaccine - Pharmacy Times Posted: 28 Feb 2019 04:06 AM PST Welcome to Throwback Thursday, Pharmacy Edition. After all of the positive feedback from fellow pharmacists who enjoyed learning about the history of soda fountains and their pharmacist inventors, we decided to start a regular weekly column, where we feature a piece of pharmacy history. As a graduate of the University of Pittsburgh School of Pharmacy, housed in Salk Hall, I thought, 'What better way to start a Throwback Thursday feature than with a tribute to Jonas Salk?'
Several years later, while on a vaccine research fellowship at the University of Michigan, Salk became an assistant professor of epidemiology. He worked closely with his mentor, Thomas Francis, Jr, who taught him the methodology of vaccine development. By 1947, Salk was appointed director of the Virus Research Laboratory at the University of Pittsburgh School of Medicine, where he began working on the early stages of a vaccine for paralytic poliomyelitis. Contrary to belief, Salk believed that his vaccine, made of "killed" polio virus, could immunize the patient without risk of infection. He tested this vaccine on a few healthy volunteers who had not had polio, including himself, his family, and colleagues—all developed antipolio antibodies and had no negative reactions to the vaccine. After national testing on 1 million children, ages 6-9 years, known as the "Polio Pioneers," it was announced in 1955 that the vaccine was safe and effective.1 In the 2 years before the vaccine was widely available, there were more than 45,000 cases of polio in the United States—this number dropped to 910 in 1962.1 Salk never patented the vaccine or earned any money from his discovery, as he preferred it to be as widely distributed as possible. With a grant from the National Science Foundation and support from the March of Dimes, he founded the Salk Institute for Biological Studies in La Jolla, California, in 1963. Salk's last years were spent searching for a vaccine against AIDS. He died at the age of 80 in 1995.1 Salk's philosophy is memorialized with his famous quote: "Hope lies in dreams, in imagination, and in the courage of those who dare to make dreams into reality."1 The Salk Institute is today home to many scientists, who conduct medical research on a variety of topics such as aging, cancer, immunology, diabetes, and more. Reference Salk Institute for Biological Sciences. History of Salk: About Jonas Salk. Salk Institute website. https://www.salk.edu/about/history-of-salk/jonas-salk/. Accessed February 27, 2019. |
| Throwback Thursday: When Winona started saying goodbye to polio - Winona Daily News Posted: 06 Mar 2019 10:14 AM PST This interview originally appeared in the Winona Daily News on Feb. 10, 1963. Next Sunday, the first of three mass clinics for oral vaccination against polio will be held in Winona. Sponsoring the project is the Winona County Medical Society, assisted by a number of other community groups and individuals. Dr. James V. Testor, chairman of the Society's polio committee, discusses the nature of Sabin vaccine and of its target, the deadly polio virus. Q: Dr. Testor, how big a project is a polio clinic such as this? A: It's pretty time-consuming. It's developing into a larger project by the day. We have several organizations now working with us plus a number of individuals. The sponsoring organization is the Winona County Medical Society. We have asked the help of the Hospital Women's Auxiliary, Junior Chamber of Commerce, Civil Defense groups and the pharmaceutical association. There probably will be 100 to 150 persons working when you add up all phases of the program. Q: For whom is the clinic being held? A: Actually it's for people of the Winona trade area. We originally started out to include only the county. But there are many people in nearby Wisconsin who get their medical services here in Winona, so the clinic was expanded to include the trade areas. People who do business in Winona will have ample opportunity to pick up forms at various business places in the city. Q: How long will it take to conduct the clinic? A: There will be three clinics at approximately six week intervals. Q: Should a person attend all three? A: That's very important. For complete immunity you must take all three vaccines. This will be one of our problems. There is always a lot of enthusiasm for the first clinic but it tends to die down for the second and third phases. This isn't a matter of additional boosters. It's three separate immunizations against three different strains of polio. It's almost as if we were vaccinating against three different diseases. To skip any one of the clinics will leave a person susceptible to one of the strains of polio.  Mr. and Mrs. Robert Hornberg of Wilson brought their nine children to a clinic at Washington-Kosciusko school for a polio clinic. Their nine children are, left to right: Ronald, Rebecca, Richard, Ruth, Raymond, Roger and Robert Jr. Mrs. Hornberg is holding Ralph and Hornberg is holding Rubin. At the table are Mrs. Gerald Schultz and Mrs. Al Dublin, volunteer clinic workers. Q: How good is the Sabin oral vaccine? A: I think it's the best available at present against the polio virus. Q: How does it compare to the Salk vaccine? A: The Salk vaccine is composed of all three types of dead polio viruses and has been very effective. The oral Sabin vaccine is a live virus vaccine, such as smallpox vaccine. It has been demonstrated to be effective against polio and in preventing the spread of polio from person to person. Q: How is polio transmitted from one person to another? A: The polio virus spreads from the hands, or by other means to the mouth and it grows in the intestines. It does not enter the body by being breathed in or though the skin or other body openings. In most people the virus is limited to the intestinal tract. Many people have had mild cases of polio and developed an immunity to it. In many cases they don't realize it because they just have a little fever and that's it. But in paralytic polio the virus breaks out of the intestines and gets into the blood stream. If no antibiotics are present it can attack the central nervous system. The Salk vaccine didn't prevent the intestinal infection but it could stop the viruses when they broke out and entered the' blood stream. It did leave one avenue of. infection open because a person could still be a carrier, even though immunized. But with the Sabin oral vaccine the intestinal tract develops an immunity, therefore the viruses can't grow there and be passed on to others. Q: Why are mass clinics held? A: By public health principles, if you can immunize a certain percentage of the population you can cut off epidemic outbreaks. If we can immunize 75 percent of the population, polio will die a natural death because it can't sustain itself among the remaining percentage. This is part of a national program to make polio a matter of past history, The tool, is here and, it's a good one. All we have to do is apply it and we will do with polio what we've done with smallpox. Q: How will the vaccine be administered? A: It's given orally. In our clinic, several drops of the vaccine will be put on a sugar cube and each person will eat one cube. This has a lot of appeal in preference to needles. Children can take it easily. In the cases of babies too small to eat the sugar cubes, the vaccine is dropped directly into their mouths. Q: Should persons previously vaccinated with Salk serum attend this clinic too? A: Very definitely. They will receive added protection and their resistance to polio will be raised. There may be a few of them who actually were not immune even though they had the Salk vaccine. By this means they will be sure, of getting the desired immunity. Q: Is polio on the increase or is the incidence declining? A: The number of cases has gone down markedly since the introduction of the Salk vaccine. In 1953, there were 53,000 cases in the country. In 1962, there were 650 cases. Q: Were medical people in this country able to profit from observation of the results of mass oral immunizations held previously in Europe? A: Yes, they were. I believe that about 100 million doses were given in Russia and other countries before oral vaccination was generally adopted here. There, are several types of the vaccine and I don't know what their results were. The Sabin type is the only one licensed for use here and it has been effective, even where epidemics have broken out, in providing quick immunity for a certain type of polio. It was first used in this country in Cleveland. In 1960 they gave over a million doses — about 76 percent of the population — and there has not been one case of polio there since that time. Q: Is the Sabin vaccine good for adults and children alike? A: It's equally effective for both. We're emphasizing it for use in children and young adults because they are the people more inclined to get polio. Q: Does polio attack greater numbers of children than adults? A: It has varied in recent years. In years past, when we had no vaccination, probably most people were exposed by the time they reached, adulthood. They either had it. or developed an immunity to it. Our prime targets now are school children and pre-school children because they are the most susceptible. About 90 million Americans already have been inoculated with Salk vaccine. Q: Can a person recover fully from an attack of polio? A: If a person had some nerve damage from an attack, he may recover some of the use if the injury is not too bad. Those who have no damage to the nervous system recover completely. But once the motor nerve cells — such as those to the arms, legs, the throat — are gone, that's it. They don't recover. Q: Will any drug stop polio, once a person gets the disease? A: No. Once you develop polio there are no drugs to cure it. Only through immunization can we actually prevent the effects. Q: Did the electron microscope provide the key to polio control by enabling scientists for the first time to actually see the virus? A: Yes, but the really big break came, in 1949 when a Harvard researcher developed a method of growing the viruses. Then science had a ready supply of them to study. Once you study them you can develop the vaccine. This was important in the development of both the Salk and Sabin-vaccines. Q: Is it preferable to give the vaccine in cold weather months? A: Yes. In cold weather there are fewer competing or interfering intestinal viruses. If we were, to have polio in the community in the summer, the thing to do would be to give the Sabin vaccine to stop a possible epidemic. But we prefer the winter for administering it when possible. Q: Will there be a fee for each dose of vaccine administered? A: We're asking a donation of 25 cents per vaccination. Our society has no funds for this activity and it will be costly. If everyone contributes a quarter, it will carry itself. Editor's note: More than 24,000 people participated in Winona's mass immunization clinics. In the May 12, 1963, Winona Daily News, just prior to the third and final clinic, medical society officials pointed to the absence of any ill effects from the 48,000 individual dosages of serum as a graphic demonstration of the Sabin vaccine's safety. |
| HISTORY, Feb. 23: US begins mass inoculations against polio - StarNewsOnline.com Posted: 23 Feb 2019 12:00 AM PST Today is Saturday, Feb. 23, the 54th day of 2019. There are 311 days left in the year. Today's Highlight in History: On Feb. 23, 1954, the first mass inoculation of schoolchildren against polio using the Salk vaccine began in Pittsburgh as some 5,000 students were vaccinated. On this date: In 1685, composer George Frideric Handel was born in present-day Germany. In 1822, Boston was granted a charter to incorporate as a city. In 1836, the siege of the Alamo began in San Antonio, Texas. In 1848, the sixth president of the United States, John Quincy Adams, died in Washington D.C., at age 80. In 1870, Mississippi was readmitted to the Union. In 1927, President Calvin Coolidge signed a bill creating the Federal Radio Commission, forerunner of the Federal Communications Commission. In 1942, the first shelling of the U.S. mainland during World War II occurred as a Japanese submarine fired on an oil refinery near Santa Barbara, California, causing little damage. In 1945, during World War II, U.S. Marines on Iwo Jima captured Mount Suribachi, where they raised two American flags (the second flag-raising was captured in the iconic Associated Press photograph.) In 1965, film comedian Stan Laurel, 74, died in Santa Monica, California. In 1998, 42 people were killed, some 2,600 homes and businesses damaged or destroyed, by tornadoes in central Florida. In 2004, the Army canceled its Comanche helicopter program after sinking $6.9 billion into it over 21 years. Education Secretary Rod Paige likened the National Education Association, the nation's largest teachers union, to a "terrorist organization" during a private White House meeting with governors. (Paige later called it a poor choice of words, but stood by his claim the NEA was using "obstructionist scare tactics.") In 2005, a jury was selected in Santa Maria, California, to decide Michael Jackson's fate on charges that he'd molested a teenage boy at his Neverland Ranch. (Jackson was later acquitted.) Ten years ago: President Barack Obama pledged to dramatically slash the skyrocketing annual budget deficit as he started to dole out the record $787 billion economic stimulus package he'd signed the previous week. Five years ago: The Sochi Olympics completed a 17-day run with Canada's 3-0 victory over Sweden in the men's hockey final, the last of 98 gold medal events. Dale Earnhardt Jr. persevered through rain and wrecks to win the Daytona 500 for the second time, a decade after his first victory in the "Great American Race." Alice Herz Sommer, 110, believed to be the oldest survivor of the Holocaust, died in London. Samuel Sheinbein, 33, who'd fled from the U.S. to Israel after murdering and dismembering a Maryland man in 1997, was killed in a shootout at an Israeli prison. One year ago: Rick Gates, a former senior adviser to Donald Trump's election campaign, pleaded guilty to federal conspiracy and false-statements charges, becoming a cooperating witness in the probe of Trump's campaign and Russia's election interference. Florida Gov. Rick Scott announced plans to put more armed guards in schools and make it harder for young adults and some with mental illness to buy guns. Teachers and staff returned to Marjory Stoneman Douglas High School in Parkland, Florida, for the first time since the shooting that left 17 people dead. Canada's Olympic men's hockey team failed to reach the final at the Winter Olympics in South Korea, losing to Germany 4-3 in the semifinals. Today's Birthdays: Actor Peter Fonda is 79. Pro and College Football Hall of Famer Fred Biletnikoff is 76. Author John Sandford is 75. Country-rock musician Rusty Young is 73. Actress Patricia Richardson is 68. Former NFL player Ed "Too Tall" Jones is 68. Rock musician Brad Whitford (Aerosmith) is 67. Singer Howard Jones is 64. Rock musician Michael Wilton (Queensryche) is 57. Country singer Dusty Drake is 55. Actress Kristin Davis is 54. Tennis player Helena Sukova is 54. Actor Marc Price is 51. TV personality/businessman Daymond John (TV: "Shark Tank") is 50. Actress Niecy Nash is 49. Rock musician Jeff Beres (Sister Hazel) is 48. Country singer Steve Holy is 47. Rock musician Lasse (loss) Johansson (The Cardigans) is 46. Film and theater composer Robert Lopez is 44. Actress Kelly Macdonald is 43. Rapper Residente (Calle 13) is 41. Actor Josh Gad is 38. Actress Emily Blunt is 36. Actor Aziz Ansari is 36. Actor Tye White (TV: "Greenleaf") is 33. Actress Dakota Fanning is 25. Thought for Today: "The essential conditions of everything you do must be choice, love, passion." — Nadia Boulanger (boo-lahn-ZHAY'), French composer and teacher (1887-1979). |
| This Is the Truth About Vaccines - The New York Times Posted: 06 Mar 2019 12:03 PM PST  Vaccinations save lives, protect our children and are one of our greatest public health achievements. As public health officials, our role is to advance the health of the American people. This must include championing vaccinations. Diseases like polio, measles, diphtheria and rubella were once common in the United States, afflicting hundreds of thousands of infants, children and adults, and killing thousands each year. Some older Americans may remember the fear associated with polio outbreaks and the era of iron lungs and leg braces — a time when swimming pools and movie theaters closed over concerns about the spread of the crippling disease. Others may recall the heartbreaking wave of rubella in the 1960s that resulted in thousands of newborn deaths, with thousands more born blind, deaf or with other lifelong disabilities. We cannot let America be faced with these fears again. For those of us who have treated critically ill children with vaccine-preventable diseases, we know firsthand the devastation to the child — and to the family and community — of a death, limb amputation or severe brain damage that could have been avoided by a simple vaccination. Modern vaccines are highly effective and safe, with most serious side effects being exceptionally rare — and much less serious than contracting the actual disease. But misinformation about vaccines is still widely reported, so we feel it is crucial to state clearly and unambiguously: Vaccines do not cause autism and they do not contain toxic chemicals. That fact was demonstrated again this week in a new study on MMR vaccination by Danish researchers. In part because vaccines have been so successful, clinicians practicing in the United States today may have never seen a patient with polio, or treated a child with measles or bacterial meningitis, and parents may not realize how severe and potentially life-threatening these diseases can be. Consider measles. The World Health Organization estimates that measles vaccination prevented more than 21 million deaths worldwide since 2000. Although routine childhood vaccination for measles remains high in the United States (greater than 91 percent for preschool children), localized dips in vaccination coverage have resulted in a recent resurgence of measles in parts of the country. A total of 17 measles outbreaks affecting more than 370 individuals have been confirmed in 2018 alone, and 10 states are already reporting cases this year. Unfortunately, many more communities are at risk for outbreaks because of areas with low vaccine coverage. Influenza continues to severely affect our families. In the last flu season of 2017-18, about 80,000 Americans died from the disease. Scores of them were children who had not been vaccinated. Yet, early season vaccination rates remain below 50 percent for both adults and children. The flu vaccine is the best way to avoid getting the disease, and those who do fall ill are less likely to develop severe flu symptoms that lead to hospitalization or death. The list goes on. In 2017, only 49 percent of American adolescents received all of the recommended doses of the HPV vaccine, which is the best way to protect both males and females from developing certain cancers — including cervical, anal, mouth and throat cancers. One in five teenagers — approximately 4.5 million people — have not received the vaccination for the contagious form of bacterial meningitis, even though the swift-moving disease can leave an otherwise healthy child facing amputation, organ failure or death within 24 hours of onset. And the nation is experiencing a multistate outbreak of hepatitis A, especially among people who use drugs or experience homelessness. Yet the disease — which can lead to liver failure and death — can be prevented with a safe and effective vaccine. We cannot be complacent. The recent measles outbreaks are a reminder that diseases that we might have thought had become rare in the United States are still infecting unvaccinated people, sometimes with dire consequences: Children with measles can develop fatal complications. These diseases should be seen only in history books — not in our emergency rooms. We are committed to countering the misinformation that fuels anti-vaccine sentiment among parents and legislators who are earnestly trying to protect their children and the public. Science that sits on the shelf has no value. We must take advantage of the lifesaving tools we have to protect our nation's most vulnerable. Our children, and our children's children, have the opportunity to grow up in a world that is free from polio, measles and other vaccine-preventable diseases. We must work together to make this a reality. Adm. Brett P. Giroir is the assistant secretary for Health and Human Services and the senior adviser for opioid policy. Robert R. Redfield is the director of the Centers for Disease Control and Prevention and administrator of the Agency for Toxic Substances and Disease Registry. Vice Adm. Jerome M. Adams is the surgeon general. The Times is committed to publishing a diversity of letters to the editor. We'd like to hear what you think about this or any of our articles. Here are some tips. And here's our email: letters@nytimes.com. Follow The New York Times Opinion section on Facebook, Twitter (@NYTopinion) and Instagram. |
| Polio this week as of 6 March 2019 - Afghanistan - ReliefWeb Posted: 07 Mar 2019 11:53 AM PST  On 26-27 February 2019, the Global Commission for Certification of the Eradication met at the World Health Organization in Geneva to continue its work on global certification criteria for wild poliovirus eradication and containment. The GCC reviewed all the latest global epidemiology and examined remaining challenges in the interruption of wild polio virus. Read more here. Featured on polioeradication.org: Coffee with Polio Experts— Dr Nicksy Gumede-Moeletsi, senior virologist at WHO's Regional Office for Africa, talks about how genetic analysis of isolated polioviruses is helping strategically drive eradication efforts in Africa. Summary of new viruses this week: Pakistan – two WPV1-positive environmental samples; Nigeria— one circulating vaccine-derived poliovirus type 2 (cVDPV2) case. See country sections below for more details. Weekly country updates as of 6 March 2019 Afghanistan No wild poliovirus type 1 (WPV1) cases were reported in the past week. There are two WPV1 cases reported in 2019. The total number of WPV1 cases for 2018 remains 21. Pakistan No cases of wild poliovirus type 1 (WPV1) were reported this week. There are four WPV1 cases reported in 2019. The total number of WPV1 cases in 2018 remains 12. Nigeria One case of circulating vaccine-derived poliovirus type 2 has been reported this week in Baruten LGA, Kwara state, with onset of paralysis on 22 January 2019. This is the second cVDPV2 AFP case reported from Kwara state. This new cVDPV2 case is the first one reported in Nigeria and globally in 2019. The total number of cVDPV2 cases in 2018 remains 34. Lake Chad Basin No case of circulating vaccine-derived poliovirus type 2 (cVDPV2) has been reported in the past week. The most recent cVDPV2 isolated in the country was in Magaria district, Zinder province with an onset of paralysis on 5 December 2018. Central Africa No cases of circulating vaccine-derived poliovirus type 2 (cVDPV2) were reported this week in the Democratic Republic of the Congo (DRC). The total number of cVDPV2 cases reported in 2018 is 20. Horn of Africa No circulating vaccine-derived poliovirus type 2 (cVDPV2) cases were reported in the past week. The Horn of Africa is currently affected by separate outbreaks of circulating vaccine-derived poliovirus type 2 (cVDPV2) and type 3 (cVDPV3), reporting both AFP cases and environmental positive samples. Papua New Guinea No new cases of circulating vaccine-derived poliovirus type 1 (cVDPV1) were reported this week. The total number of cases in 2018 remains 26. Mozambique No case of circulating vaccine-derived poliovirus type 2 (cVDPV2) outbreak has been reported this week. The total number of cases in 2018 remains 1. Indonesia No circulating vaccine-derived poliovirus type 1 (cVDPV1) cases were reported this week. Two genetically-linked circulating vaccine-derived poliovirus type 1 (cVDPV1) isolates were detected, from an acute flaccid paralysis (AFP) case, with onset of paralysis on 27 November 2018, and from a sample of a healthy community contact, in Papua province collected on 24 January 2019. This outbreak is not linked to the cVDPV1 currently affecting neighbouring Papua New Guinea. |
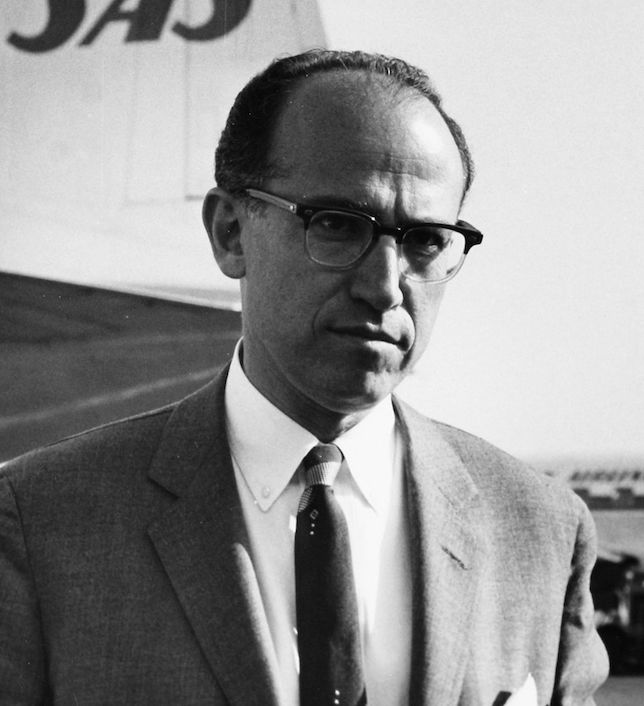 Jonas Edward Salk was born in October of 1914, in New York City.1 The eldest of 3 sons, he was the first member of his family to attend college. In 1939, he earned his medical degree from the NYU School of Medicine and worked as a scientist physician at Mount Sinai Hospital.1
Jonas Edward Salk was born in October of 1914, in New York City.1 The eldest of 3 sons, he was the first member of his family to attend college. In 1939, he earned his medical degree from the NYU School of Medicine and worked as a scientist physician at Mount Sinai Hospital.1| You are subscribed to email updates from "polio history" - Google News. To stop receiving these emails, you may unsubscribe now. | Email delivery powered by Google |
| Google, 1600 Amphitheatre Parkway, Mountain View, CA 94043, United States | |



Comments
Post a Comment